CME
Physicians: Maximum of 1.00 AMA PRA Category 1 Credit™
Released: May 27, 2025
Expiration: November 26, 2025
LAURA: Osimertinib vs Placebo After Definitive Chemoradiotherapy for Unresectable Stage III EGFR-Mutated NSCLC
I start by discussing 2 studies from ELCC 2025 for the treatment of EGFR-mutated NSCLC, one of which is the randomized phase III LAURA study. This trial tested osimertinib (n = 143) vs placebo (n = 73) for the treatment of patients with locally advanced, unresectable stage III NSCLC with EGFR mutations (Ex19del or L858R) after chemoradiotherapy (with no disease progression during or after treatment). The primary analysis showed an impressive improvement in PFS (9.1 vs 5.6 months with placebo; HR: 0.16) and led to FDA approval for this patient population.1,2 Osimertinib is now considered the standard-of-care (SoC) first-line treatment for this patient population. The interim OS data at 20% maturity had a positive trend in favor of osimertinib vs placebo post chemoradiotherapy.1 The updated OS results were reported at ELCC 2025.
LAURA Updated OS: Baseline Characteristics
The population included in LAURA represented the classical characteristics of patients with locally advanced EGFR-mutated NSCLC.3-5 For instance, this was a primarily young population with a median age of 62-64 years in both the osimertinib and placebo arms. There was also a slight majority of female patients (63% in the osimertinib arm and 58% in the placebo arm). Also, more patients had 60% of patients had Ex19del (52% and 59%) than L858R mutations of EGFR (48% and 41%), which is what we expect from this population.
Patients were primarily never smokers (71% and 67%) or former smokers (26% and 32%) and had histology reflecting adenocarcinoma (97% and 95%). The final aspect was that most patients received the SoC concurrent chemoradiotherapy (92% and 85%).
LAURA Updated OS: Patient Disposition and FST
The updated OS data were taken with a median follow-up of 39.4 months and 35.2 months in the osimertinib and placebo arms respectively.3 Yet, these were still immature (31% maturity), so we will need further data to confirm whether there is an OS benefit with osimertinib.
Of note, crossover was permitted and 77% of patients in the placebo arm received osimertinib treatment after discontinuing the placebo. This means that if the final OS data are positive, then it is clear that osimertinib treatment should be started immediately after chemoradiotherapy instead of traditionally waiting for progressive disease to start osimertinib.
LAURA Updated OS: Interim and Updated OS Results
The immature intermediate OS results had an HR of 0.81 which was not statistically significant (P = .530) but showed a positive trend toward osimertinib treatment.3 We will need to wait longer for more mature and conclusive data, but the updated results still confirm the positive trend in favor of osimertinib with an improved HR of 0.67 (P = .140).
LAURA Updated OS: Postprogression Endpoints TFST, PFS2, and TSST
The postprogression data should be cautiously considered because they are secondary endpoints, but they also generally support the benefit of osimertinib following chemoradiotherapy. The time to first subsequent treatment is substantially higher for the osimertinib arm vs the placebo arm at 43.8 months vs 9.5 months (HR: 0.13; P <.001).3 PFS after the first subsequent treatment (PFS2) also favors osimertinib vs placebo with an HR of 0.62 (P = .088). These results further suggest that we may see positive final OS results.
LAURA Updated OS: Conclusions
This updated data for the LAURA study show further benefit of the SoC osimertinib treatment post chemoradiotherapy for patients with unresectable stage III EGFR-mutated NSCLC before disease progression occurs.3 There is a positive trend in OS data and postprogression outcomes, particularly time to first subsequent treatment and PFS2, also show a benefit for starting osimertinib soon after chemoradiotherapy. However, final OS results are needed to make this the SoC strategy rather than starting osimertinib therapy after disease progression.
MARIPOSA: Amivantamab Plus Lazertinib vs Osimertinib for First-line Treatment of EGFR-Mutated NSCLC
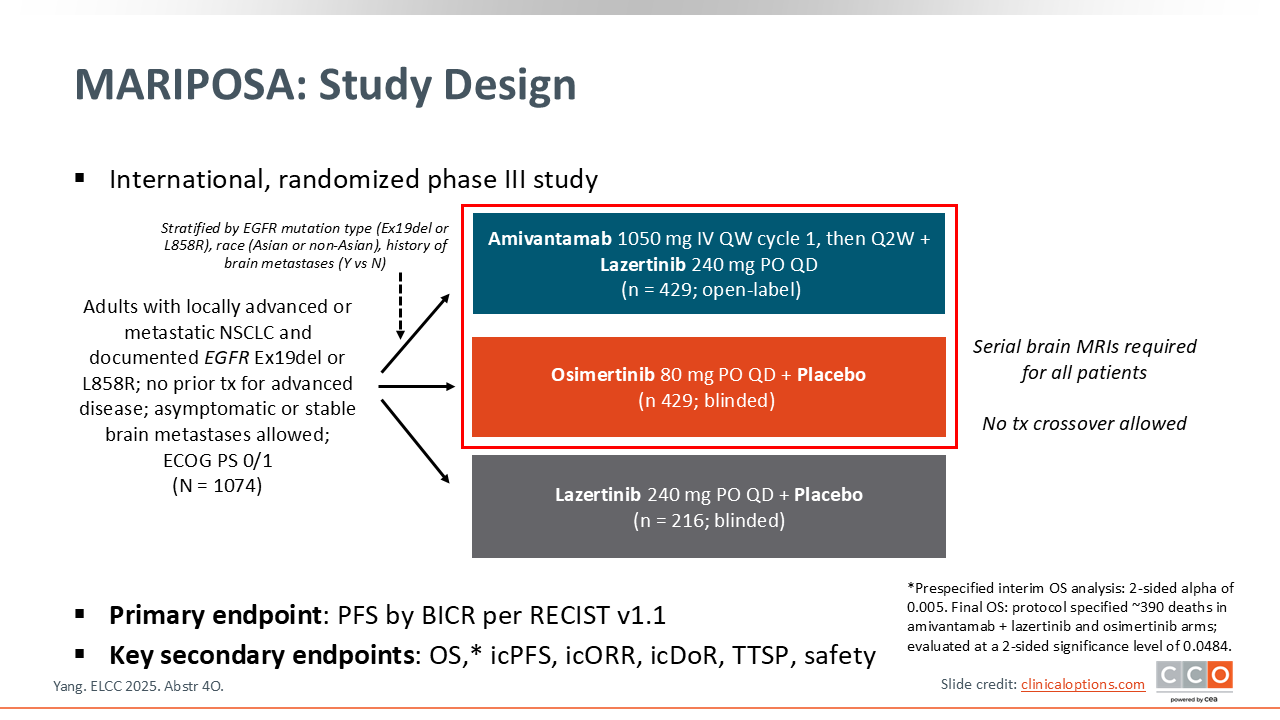
The phase III MARIPOSA trial randomized previously untreated patients with locally advanced or metastatic NSCLC and EGFR mutations, Ex19del or L858R, to the combination treatment of amivantamab plus lazertinib (n = 429) vs the first-line SoC osimertinib (n = 429) vs lazertinib plus placebo (n = 216).6 Previously published data show significantly improved median PFS for amivantamab plus lazertinib vs osimertinib (23.7 vs 16.6 months; HR: 0.70; P <.001), which led to European Medicines Agency and FDA approval of amivantamab plus lazertinib for first-line treatment of this patient population.7-11 Yet to become the new SoC, this combination must also demonstrate improved OS, a coprimary endpoint.
Yang and colleagues presented the final OS data of this study at ELCC 2025, which showed superior median OS for amivantamab plus lazertinib compared with osimertinib monotherapy.6
MARIPOSA: Baseline Characteristics
This study also included a classical population of patients with locally advanced or metastatic EGFR-mutated NSCLC with a median age of 63-64 years.6 There was also a slight majority of female patients (64% in the combination arm and 59% in the osimertinib arm) and patients with Ex19del (60%) vs L858R mutations (40%).
Of importance, approximately 40% of patients had a history of brain metastases. We know that osimertinib is highly effective for treating brain metastases, so it is also important to evaluate the efficacy of the newer combination therapy in this population.12
MARIPOSA: OS
Interim OS analysis of MARIPOSA showed a trend in improvement for amivantamab plus lazertinib vs osimertinib (HR: 0.80), but the final analysis confirms a statistically significant improvement with median OS not reached for the combination vs 36.7 months for osimertinib (HR: 0.75; P <.005).6,7 We can see in this figure that the OS Kaplan-Meier curves continue to diverge over time with a projected median OS benefit of >1 year.
MARIPOSA: Predefined Subgroup Analysis of OS
In addition, there appears to be an OS benefit across different subpopulations defined by sex, race, and history of brain metastases.6 However, there is not a clear benefit for older patients, particularly patients older than 65 years of age (HR: 1.11), and patients with L858R mutations (HR: 0.90).
MARIPOSA: First Subsequent Therapy
It is also important to examine the subsequent treatment of these patients after relapse post first-line treatment. Most patients after either amivantamab plus lazertinib or osimertinib received chemotherapy-based treatment, which I would say is the SoC in this population, particularly after these first-line treatments.6
Of importance, approximately 25% of patients did not receive a second line of treatment and there was no treatment crossover. This means that patients who relapsed after osimertinib did not receive amivantamab in combination with chemotherapy in the second line which is the SoC in this setting.
MARIPOSA: Intracranial Efficacy
As I mentioned it is important to consider the intracranial efficacy of these agents. The intracranial ORR appears to be comparable between the 2 arms with an ORR of 78% for amivantamab plus lazertinib and 77% for osimertinib.6 The median intracranial PFS is slightly improved with the amivantamab plus lazertinib vs osimertinib (25.4 vs 22.2 months), but this improvement was not statistically significant (HR: 0.79; P = .07). Median intracranial DoR was also improved (35.7 vs 29.6 months).
MARIPOSA: Safety
The combination of amivantamab plus lazertinib was associated with an increased rate of adverse events (AEs) compared with osimertinib, particularly AEs related to EGFR inhibition such as paronychia (69% vs 30%) and rash (64% vs 32%).6 AEs related to MET inhibition are also more common, like hypoalbuminemia (51% vs 7%) and peripheral edema (38% vs 7%). Because amivantamab is administered intravenously, we see a 65% incidence of infusion-related reactions with the combination therapy compared with 0% for the oral osimertinib. In addition, venous thromboembolism occurred in 40% of patients with amivantamab plus lazertinib vs 11% with osimertinib. For patients receiving the combination therapy, I would recommend prophylactic medications, like anticoagulants, to prevent these AEs.
MARIPOSA: First Onset of Key AEs for First-line Amivantamab Plus Lazertinib
The study investigators also presented the timing of the first onset of AEs, which shows that AEs primarily first occur within the initial 4 months of treatment.6 The cumulative AE incidence or the duration of these AEs would better reflect the tolerability of the combination of amivantamab plus lazertinib but was not reported.
MARIPOSA: Prophylaxis for Early-Onset AEs
It is possible to prevent some of these AEs, such as dermatologic AEs, infusion-related reactions, and venous thromboembolism. The phase II COCOON study showed that dermatologic AEs could be reduced among patients treated with amivantamab plus lazertinib with oral doxycycline or minocycline, clindamycin lotion for the scalp, chlorhexidine to wash the hands and feet, and moisturizer.13 This regimen reduced grade ≥2 dermatologic AEs from 76.5% with the SoC dermatologic management to 38.6%.
For infusion-related reactions, the phase II SKIPPirr trial showed that twice daily 8 mg of dexamethasone reduced the rate of incidence from 67.4% with standard management to 22.5%.14 Another study found that prophylactic anticoagulation reduced the incidence of venous thromboembolism in patients treated with subcutaneous amivantamab and oral lazertinib from 20.0% to 11.4%.15
MARIPOSA: Conclusions
The MARIPOSA study showed that the combination therapy of amivantamab plus lazertinib increased the median PFS of patients with EGFR-mutated NSCLC compared with the SoC treatment, osimertinib.6 The final OS results presented at ELCC 2025 also showed a significant improvement in median OS, although no treatment crossover was allowed. This means that patients who relapsed after osimertinib did not receive amivantamab in combination with chemotherapy in the second line, which is the SoC in this setting. It is unclear what OS results would be with this standard treatment for the osimertinib arm.
This combination also demonstrated potentially improved efficacy for brain metastases in this patient population. However, the magnitude of the benefit for intracranial PFS and intracranial DoR is not definitive. Further data, particularly the complete intracranial brain response rate, would help define the benefit for treating brain metastases.
In addition, despite the improvement in OS, amivantamab plus lazertinib results in a significant impact on patient quality of life due to increased AEs such as dermatologic AEs, infusion-related reactions, venous thromboembolism, and peripheral edema. There are prophylactic regimens that can help prevent these AEs, but they can involve many treatments and do not eliminate risk of developing the AEs. So I think it may be challenging to convince healthcare professionals to adopt this combination therapy regimen as a new SoC for first-line treatment of EGFR-mutated NSCLC.
Furthermore, these results should be considered alongside those of the phase III FLAURA2 trial. FLAURA2 has demonstrated a significant PFS benefit for osimertinib with chemotherapy vs osimertinib monotherapy for the first-line treatment of the same patient population (median PFS: 25.5 vs 16.7 months; HR: 0.62; P <.001).16 Osimertinib with chemotherapy appears to benefit patients with brain metastases (24.9 vs 13.8; HR: 0.47) and the L858R EGFR mutation (24.7 vs 13.9; HR: 0.63) in particular.
In my opinion, the MARIPOSA regimen may be best adopted for the treatment of select patient subpopulations that receive the most benefit. For instance, there was a positive trend in OS benefit with this regimen for patients with Ex19del, but the trend was less clear for those with the L858R mutation.6 There may be other biomarkers like circulating tumor DNA positivity or MET amplification that may identify patients who are likely to benefit from amivantamab plus lazertinib. It is also possible that the regimen has too much toxicity to be an effective treatment for patients 65 years of age or older.
Further study will be needed to identify the patients who would most benefit from amivantamab plus lazertinib rather than osimertinib. In the meantime, I believe osimertinib will remain the SoC given its general benefit and better tolerability.